
VOO, AOO, OHNOO!
- Sam Ireland
- Nov 24, 2017
- 5 min read
Pacemakers are such interesting devices! I just read an article about the smallest pacemaker ever, the "Micra." It's wireless, and leaves the patient free from scars and the classic upper left chest (or wherever else) pacemaker implantation. It looks like a pill with hooks. It is hooked directly into the ventricular wall, and can stay there for up to 12 years! Wow!

In emergency and critical care, pacer modes can be difficult to remember and deal with. I wanted to make this blog not only to explain what I know about them (which isn't really much), but also to create a resource for anyone to reference when they have a pacemaker issue they are trying to resolve. Let's start with figuring out the different modes!
Interpreting Pacer Modes
The letters that describe a pacer mode have a key that shows us what each letters means.

With the key, it is now very simple to interpret what the letters in a pacer mode mean. For example, check out VVI:
V - The ventricle is the area of the heart where the pacer makes contact and paces from.
V - The pacer senses if the ventricle has it's own intrinsic beats
I - What does the pacer do if it senses that the ventricle originates its own beat? The pacer is inhibited (it does not send a signal, since the ventricle did it on its own).
Let's take a look at what some of the common modes would look like on a rhythm strip.
AOO
Paced: Atrium / "A"
Sensed: None / "O"
Response to sensing: None / "O"
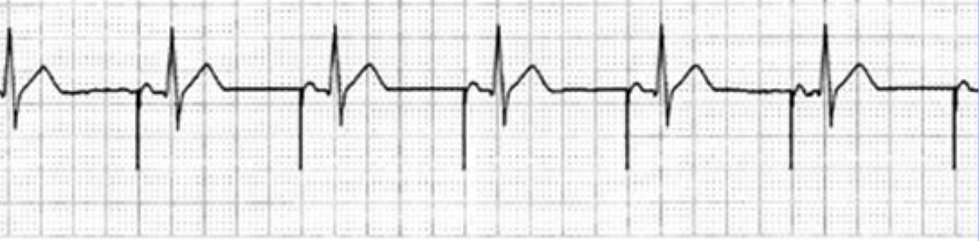
AOO is atrial paced, with no sensing. For this pacer mode to work for someone, they must have a good electrical connection between the atria and ventricle. This mode would not work for a patient with a high degree AVB for obvious reasons.
VOO
Paced: Ventricle / "V"
Sensed: None / "O"
Response to sensing: None / "O"

VOO is ventricular paced, with no sensing. Examine the above rhythm strip. Does something look very wrong? We'll get to that in a little bit.
DOO
Paced: Atria and ventricle / "D"
Sensed: None / "O"
Response to sensing: None / "O"

DOO will pace the atria with one lead, while another lead sits in the ventricle and paces there as well. There is a programmed delay set in the pacemaker that acts like an AV node. This allows adequate time for the 'atrial kick' to fill the ventricles.
VVI
Paced: Ventricle / "V"
Sensed: Ventricle / "V"
Response to sensing: Inhibited / "I"

VVI paces the ventricle when needed, and senses when the pacer is not needed. When the pacer senses an intrinsic beat, it should not fire.
DDD
Paced: Atria and ventricle / "D"
Sensed: Atria and ventricle / "D"
Response to sensing: Atria and ventricle inhibited and triggered / "D"

DDD is a mode that can pace both the atria and ventricle, and sense both as well. The 'response to sensing' function on the DDD mode is very interesting. It can either be inhibited, or triggered. If you study the above rhythm strip, you will see what I mean. If the heart starts with a P wave, the pacer can inhibit the atrial lead, and trigger the ventricular lead if the heart does not follow through with a QRS (and the other way around).
What about the fourth and fifth letters in the pacer code? You may not be able to immediately tell if these functions are active just by looking at a rhythm strip. If the pacemaker can be influenced by various signals from the patient to increase its firing rate, it may have an "R" as its fourth letter, etc. One thing you may be able to tell is if there is a fifth letter. How?
If the pacemaker can function as an implanted cardiac defibrillator, this would be a fifth letter of "S." If the pacemaker can also do "anti tachyarrhythmia" pacing, you will see this on an ecg. It's called "ATP" for "Anti Tachycardia Pacing" If the pacemaker has both shocking and ATP functions, the fifth letter would be a "D."
Here is an example of ATP. The pacer paced at a rate above the intrinsic arrhythmia, and then brought the rate down. Pretty cool!

Pacer Magnets
I've noticed that there is some confusion surrounding pacer magnets and their effect on a pacemaker. Basically, the pacer magnet turns the pacer into a non-sensed mode. When a pacer magnet is applied, here is how it would change the modes:
DDD would turn into DOO
VVI would turn into VOO
AAI would turn into AOO
How does the pacer magnet accomplish this? It has a switch inside that is activated by the magnet. Check it out:

Once the leads inside the Reed Switch touch, it changes the pacer into a non-sensed mode. This makes the pacer fire at its "Rate*," which is a pre-programmed rate that is set within the pacemaker. Once the magnet is removed, the pacemaker changes back to its regular, everyday mode. This can be a useful diagnostic or treatment tool if you suspect the pacer is not performing properly.
Cardiac Axis and Pacemakers
I recently posted a blog about cardiac axis. In that blog, I mentioned that saying a pacemaker will always have a pathological left axis deviation was an oversimplification. This is because a pacemaker should really only produce pathological left axis deviation of the QRS if the pacing lead is in the apex of the R ventricle. There is apparently now starting to be a push to place the pacing lead in the right ventricular outflow tract (RVOT). I am not a cardiologist, so I can only repeat what I read about this. Apparently, placement of the pacer lead at the RVOT may reduce risk of heart failure, and help prevent ventricular dyssynchrony. What is interesting about this placement to me, is that it produces a different mean axis. Here is a picture that illustrates how pacer lead placement may alter cardiac axis in the frontal plane:

Don't Forget Smith Modified Sgarbossa Criteria!
If you have a patient that you suspect of having a cardiac event (and has a pacemaker/LBBB/LVH), you should check for Smith Modified Sgarbossa Criteria. If the patient has a mode that only paces the atria, like AOO, you can assess for regular STE. However, in patients with a wide complex, ventricular paced rhythm, you need to use the Smith Modified Sgarbossa Criteria. Here is a quick graphic I made to reference the criteria:

Pacemaker Syndrome
Remember when we were looking at the VOO pacer rhythm strip above, and I asked if you noticed something very wrong about it? Last chance to guess if you haven't examined the rhythm strip closely yet!
...
Notice the P waves? Those are wasted P waves. That patient has good atrial function, but is being robbed of their atrial kick because they do not have a dual-lead pacer that allows them to synchronize the atria and the ventricle! For shame! This can contribute to something called "pacemaker syndrome." This syndrome is a set list of possible side effects that can come from pacer initiation of any kind (transthoracic, transvenous, or implanted). It basically has to do with AV dyssynchrony caused by inappropriate pacer timing as related to intrinsic atrial activity. The atrial kick can contribute 15-30% of CO, according to some sources. That's a lot! This is why chemical pacing, or dual-lead pacing is prefered in patients who have working an atrium that is able to contract normally (no atrial fibrillation or flutter). I won't go into depth on pacemaker syndrome here, but I encourage you to research it for yourself. I'll provide some links below. It is very important to think about atrial kick when we are deciding between the electronic pacer and the epi drip. Different rhythms will respond better to different treatments. Do not think of bradycardia as a blanket term, you must think about AV synchrony when deciding on a treatment. Avoid causing Pacemaker Syndrome!
Resources and references:
https://lifeinthefastlane.com/ccc/pacing-modes-advantages-and-disadvantages/
http://www.pacemaker.vuurwerk.nl/info/nbg_code__naspe.htm
http://www.medtronic.com/us-en/patients/treatments-therapies/pacemakers/our/micra.html
https://emedicine.medscape.com/article/159706-overview
https://www.911tacmed.com/uploads/4/0/4/0/40402475/cardiac_output.pdf
https://bjcardio.co.uk/2008/01/pacemaker-syndrome-a-forgotten-diagnosis/
https://drsvenkatesan.com/2013/11/16/what-is-the-role-of-magnet-in-pacemaker-evaluation/


